
 Locations
Locations

About 2 out of every 10 children live in households that may be characterized as being structurally poor in Argentina.
Note: This blog is part of Lustig, N. & Tommasi, M. (2020). El COVID-19 y la protección social de los grupos pobres y vulnerables. UNDP. (Forthcoming)
A pandemic or an epidemic acts on the wellbeing of the population through various channels. In some cases, by having a direct impact on the health of an active member of a household and reducing their income-generating capacity and, therefore, lowering the level of wellbeing. But there are other more indirect ways that are equally important. The containment phase for any pandemic or epidemic (which includes isolation, quarantine, and school closings) has a recessive effect on economic activity, which has a negative impact on the labor market and public finances, among other economic dimensions, and ends up affecting the wellbeing of households and the people comprising them.
Children in the care of older people who are affected are adversely affected for these reasons as well. But they also face the added impact of not being able to go to school. According to the latest data available from Ministry of Education statistics, in Argentina there are approximately 10,491,524 girls and boys who attend school at the primary and secondary school levels. This represents 79.6% of the population under 18 years of age.
The effect that these factors may have on wellbeing will depend on preexisting vulnerability conditions, some of which are very specific and concrete, and many others that cannot be determined from the information available from household surveys.
Preexisting conditions of vulnerability
Just as the novel coronavirus causes mortality in older people due to certain preexisting health conditions (primarily hypertension, diabetes, and obesity), preexisting social conditions can have an impact on the wellbeing of the population. In the case of children, preexisting social conditions arise from their individual circumstances (school attendance, for example), from the circumstances of the adult person responsible for their care, or from the household where they reside.
Moreover, the mechanisms or channels through which this occurs may be both direct and indirect. The direct ones adversely affect the health of the population; the indirect ones are due to the measures that the government must take in order to deal with the pandemic. The effects of such impacts on wellbeing could be mitigated through concrete public policy actions, often using preexisting social protection programs, to counter declines in wellbeing.
Direct transmission channels are those that directly permeate, without mediation, the conditions that determine the wellbeing of a child or adolescent. For example, the illness or death of a household income recipient, caused by the virus. In the case of death, there is no need for further explanation, but the disease can also result in a loss of income, working days, or employment.
Indirect transmission channels originate from measures imposed by the government, such as a lockdown, or from economic crisis, and do not differ in their effects from the traditional ones. It is emphasized that these are government measures that are motivated by the need to contain (and/or mitigate) a pandemic or an epidemic that a government must necessarily implement, which cause serious problems. An example is the fall in aggregate economic activity and its effects on employment and on the population’s income.
Vulnerabilities detected
Children and adolescents face various risks in the face of the COVID-19 pandemic, especially those living in households where the head of household or reference person (RP) is a woman.
The risks of seeing the circumstances for their wellbeing deteriorate affect an important group of children and adolescents in the country. The percentage of children in preexisting situations of vulnerability according to the indicators used ranges from 28% to 63% in all households and from 30% to 72% in households headed up by women.
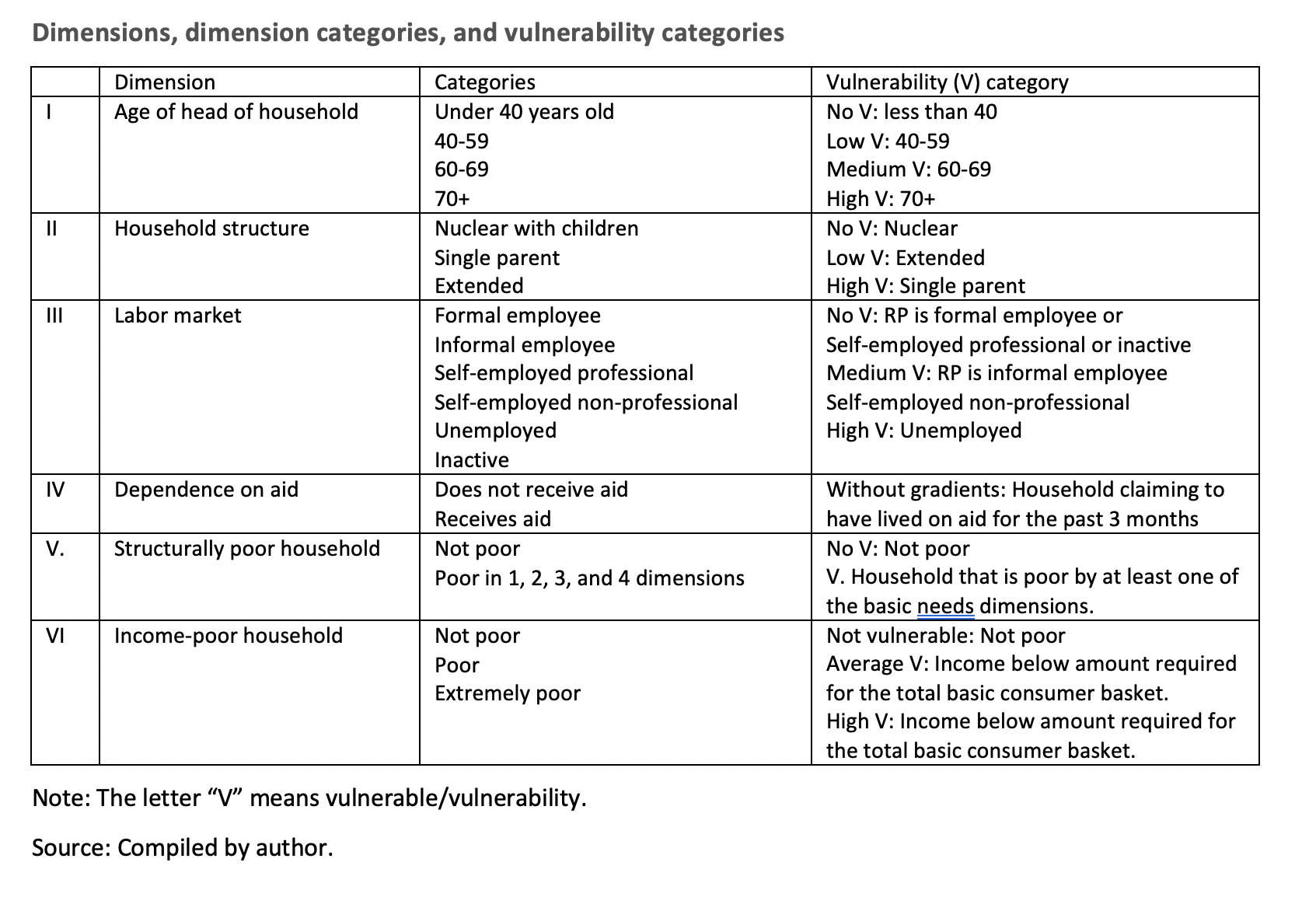
No significant differences by sex were found. For households in general, the highest vulnerability is detected for multidimensional-union poverty and the lowest for structural poverty.[1] In female-headed households, the greatest vulnerability comes from the labor market and the lowest, as in the previous case, from households that are poor due to Unsatisfied Basic Needs (UBN).
More than half of all children live in households where the head of household or reference person (RP) has a positive probability of dying. This proportion is unevenly distributed over the national territory, being greater in the northwest and in the northeast, and in the eastern strip going up to the first half of the national territory.
The probability of dying is positive after 40 years of age. The evidence is the same as what is found in studies done for other countries, as well as direct unprocessed data from countries with an early onset of the pandemic.
Between 56% and 58% of all children in Argentina live in homes with some type of mortality risk for their RP. In addition, the cited percentages are markedly reduced as the age of the RP increases.
Children who are at risk due to type of household account for over 40% in general, but over 60% for those where the RP is a woman. This is the case because most single-parent households are headed by women. Consequently, the proportion of children in female-headed single-parent households is more than double the average. In this case, there are both economic and care risks. If the mother works, the children have to be left alone; if the mother spends her time caring for them, the household income may fall and place the material livelihood of the household at risk. Overall, around 1.5 million children are in this situation (female-headed single-parent households).
The concept of an extended-family household at risk is less intuitive. These households have many members and include several generations. Their vulnerability is probably captured by other indicators, such as poverty from UBN (mainly overcrowding) or the age of the RP. An example of the latter are households headed by an elderly person, who has a higher risk of mortality.
More than half of all children live in households where the head of household is unemployed or faces precarious circumstances in the labor market. This percentage surpasses 70% when there is a female head of household. This is a risk associated with both occupational and income stability. The possibility of their participation in the labor market being interrupted or of receiving irregular income increases the probability of monetary and even non-monetary poverty, if this makes it impossible to face rental costs, for example, and they have to move to an extended-family household.
Half of the children in the country live in households that say they have lived off aid from different organizations, mainly the government. This aid includes not only monetary aid, but also goods, clothing, food, etc., and not only from the government but also from other institutions: relatives, neighbors, or other people who do not live in the same household.
About 2 out of every 10 children live in households that may be characterized as being structurally poor. Note that this indicator represents the population under 18 years of age living in overcrowded conditions, in precarious dwellings, due to the construction materials used, and in housing without a bathroom. If there is a bathroom, they have no drainage or no access to potable drinking water. It also includes indicators for school attendance. All of these factors hamper application of the preventive actions suggested by health agencies whose mission is to contain the pandemic.
The territorial distribution of this phenomenon should be noted. The largest number of structurally poor children are concentrated in the areas with the largest populations, but the highest proportion is found in the traditionally poor areas of the country: the Northwest and Northeast, and the departments of the southern provinces of the country.
More than half of all children live in households with insufficient income. The scarcity of monetary resources has an impact on all dimensions of wellbeing: the possibilities for education, access to medicine, proper nutrition, etc. Furthermore, this shows that despite the extensive coverage of current social protection programs and their precise targeting, they are not sufficient to cover family budgetary needs. These figures may increase due to the connection between this dimension and others analyzed herein: principally single-parent households and difficulties related to the labor market.
The seriousness of the situation can be assessed by the number of vulnerabilities faced by a child or adolescent. The number of children who do not face any kind of risk is very low in Argentina: 8.6%. The rest of the population under 18 years old faces some type of vulnerability. The number is also low for those who confront six vulnerabilities all together: 2.9%. Vulnerability originating in the labor market is clearly the one with the greatest weight.
Conclusions and agenda
Due to preexisting social and economic conditions, the country’s children constitute a population at risk from the pandemic. Based on the indicators examined, more than half of all children may be in conditions of social vulnerability. This means more than 2.5 million children under 18 years of age. This figure is even higher when the interrelated impact of all the dimensions considered herein is taken into account.
It remains for future inquiries to assess the effect of school non-attendance in relation to the resources available in the home. Internet connectivity and availability of an access device (a home computer) is key in this regard. The starting point for such an investigation is an intuitive idea that is thought to be true: the negative effect of isolation can be partially mitigated if children have access to these alternatives. In this sense, the lack of connectivity and of the means to access connectivity represents a vulnerability factor in the current health crisis.
In this regard, still preliminary evidence shows that in the lowest quintile of family income, 75% of children do not have computers at home and 36% do not have internet access. These figures contrast sharply with those for children in quintile 5: 5% without computers and 2% without internet access.[2]
[1] To understand the dimensions involved in multidimensional poverty, see Paz (2019).
[2] This data comes from the Encuesta Permanente de Hogares (EPH) Access and Use of Information and Communication Technologies Module, 4th quarter of 2018.
